
The growth of midlevel providers has been explosive compared to physicians. This growth has lead to many young physicians, residents, fellows, and med studies worried about what their future holds. Midlevel providers can provide wonderful access to patient care. I know many amazing midlevel providers who I have worked with in the past. This article is not here to be a bashing echo chamber to hate on midlevels. So, if that is what you are expecting, you might as well stop reading now.
What this article is meant to convey, is what I believe midlevel encroachment means for physicians. How this will affect physicians daily life in the office, how we practice medicine, and the financial implications of this. I view the current rise in midlevel scope somewhat like the rise in online shopping. In the beginning, it has its fringe uses (midwives). As time grew, it rapidly becomes more ever present in our everyday life. Midlevels are clearly here to stay. Physicians will need to adapt to the changing market.
The Status Of Midlevels Where I Live
As one of my previous mentors would say, anecdotal data is one step above pure junk. I still hold onto the thought that anecdotal accounts are not worthless though! So, lets get this out of the way early….then get to the actual data.
I moved to the current city I live in about 4 years ago. In that time, I can not recall a single psychiatric outpatient referral of mine who has actually seen a physician for their entire visit. It seems my patients have only been seen by midlevel providers. About 50% of my referrals to endocrine, rheumatology, dermatology are also seen by midlevel providers based on the notes that I receive back from medical offices.
In the past 4 years I’ve watched as my local market has been flooded with midlevel providers who are now seeing many of my outpatient referrals. When I send a patient to GI, endocrine, dermatology, pulmonary, and one of the HIV clinics, the patients are often times seen by the midlevel rather than a physician.
Yes, many patients of mine are still seen by a physician. This is especially true for surgical specialties. Many of my patients with a complicated problem are still seen by a physician. However, more and more I am seeing notes written by midlevels rather than physicians for my patients. The local HIV clinic is only staffed by midlevels. The overseeing doctor does not even live in the city where I’m located according to the practice website. The same is true about several local med-spas and most of the urgent cares nearby also.
The Rise Of Online Nurse Practitioner Schools
According to Nurse.org, there are currently 521 online schools where one can obtain their NP degree online. Let that sink in. Over 500 schools to get a degree to practice medicine as a NP. Keep in mind that there are currently 190 medical schools listed in the United States.
The boom of online education and the acceptance of an online degree for practicing medicine for NP’s has lead to an explosion of nurses who want to advance their education and make more money while still keeping their day job.
I don’t blame nurses. The desire to grow ones education and provide more for their family is a noble cause.
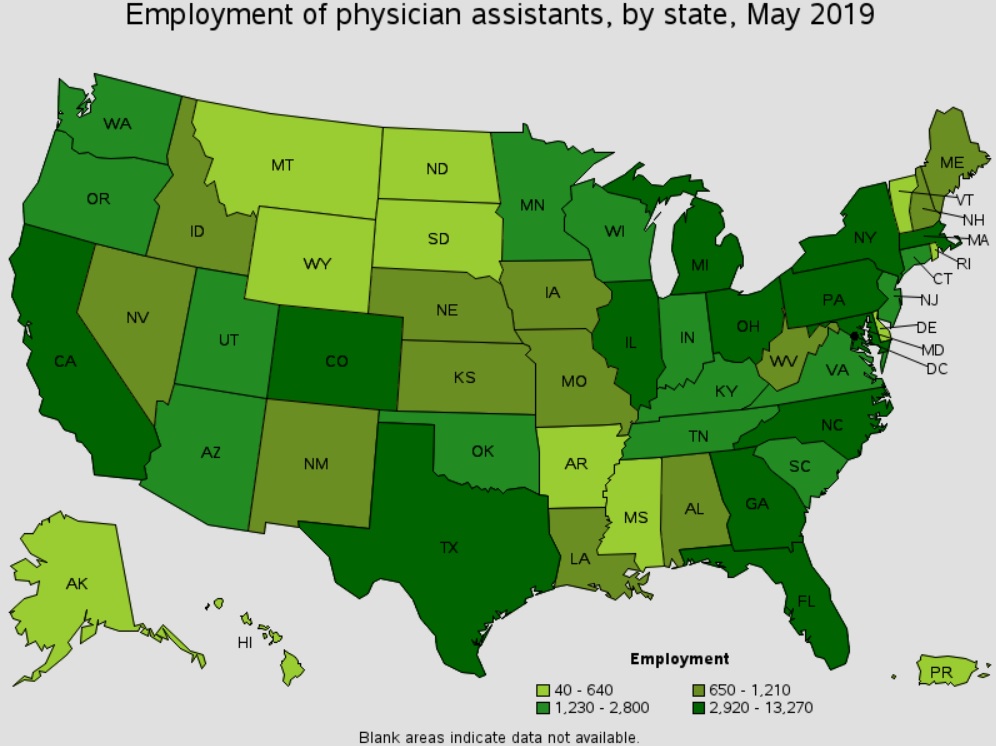
Lets take a look in the growth of employment in NP’s in the past 4 years. All data is based from the government labor and statics website for May of each year.
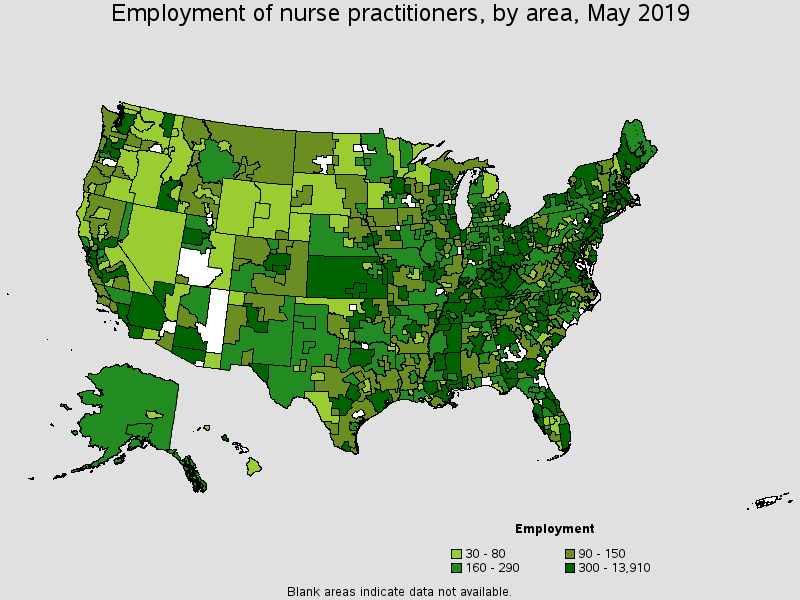
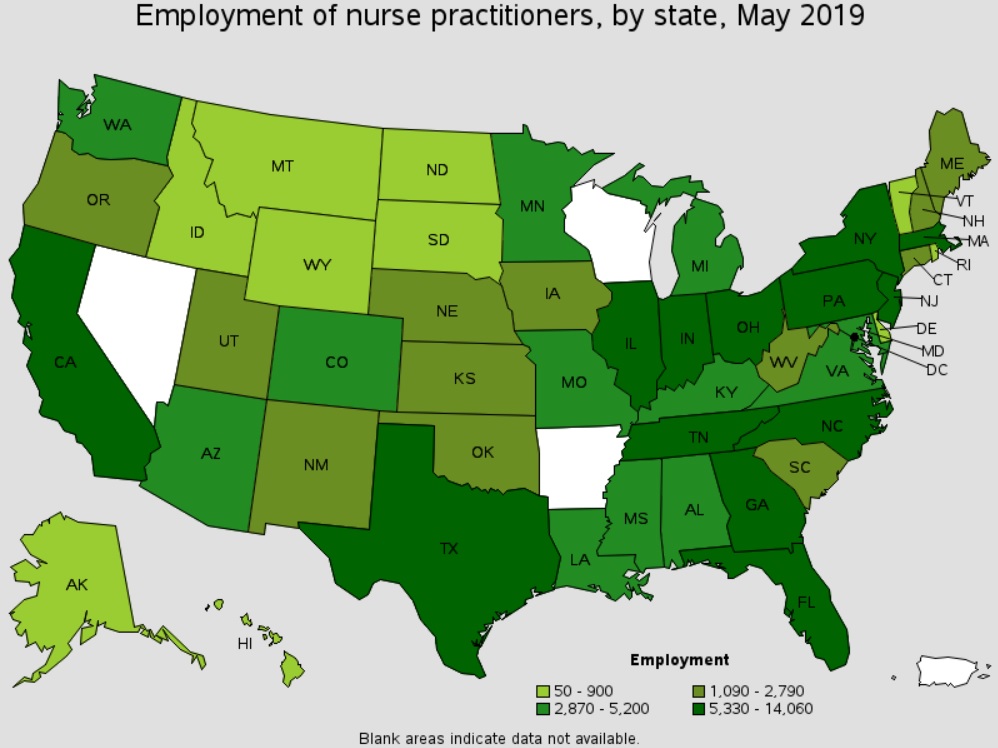
Rise In Subsequent Employment Of Nurse Practitioners
| Year | Number of Nurse Practitioners | Mean Annual Wage |
| 2016 | 150,230 | 104,610 |
| 2017 | 166,280 | 107,480 |
| 2018 | 179,650 | 110,030 |
| 2019 | 200,600 | 111,840 |
Since 2016, there has been a 34% rise in the number of employed nurse practitioners. At the current rate, the number of nurse practitioners will double in about 7 years. The same amount of time a new medical student will go from entering medical school to graduating internal medicine, family medicine, or any other 3-4 year residency options.
A medical student starting med school in 2020 can expect an extra quarter million NP’s employed by the time they graduate assuming this growth continues.
I suspect growth will hit a wall though. According to the government website for statics and labor, in May 2019 there are currently 685,830 physicians working in the United States. It is hard to believe that the market can absorb a quarter million new NP providers in the next 7 years on top of the now 200,000 currently in the workforce.
The Perfect Storm
Access to healthcare has been a huge issue. Lets take a look at the reasons behind the growth in midlevels.
- States allowing independent practices of nurse practitioners
- Currently 22 states allow for NP’s to have independent practices of medicine
- Independent groups selling out to large groups or Venture capital backed groups
- These groups are maximizing profit. It is much more cost effective to pay a NP while still submitting insurance claims and pocket the profit
- Strong NP lobby while AMA has arguably become loathed by most physicians. AMA now has a perception of focusing more on collecting fees rather than lobbying for doctors. I actually don’t know a single person who is a member of the AMA.
- Physicians stepping out of administrative roles and allowing non physicians to lead
- The increase in pay from nurse to NP. Continue to go to school online and still work at the same time to avoid increased debt load makes this avenue very attractive. Life does not need to be placed on hold like for residency.
Are We Nearing Saturation?
I do not have an advertisement out for a job posting for a new physician or midlevel to join my group. Despite this, each week I get about 2 unsolicited applications for a NP to work for me in my clinic.
I also get another 2-4 people a week email us asking if they can do their clinical rotations for their degree to become a NP. It brings up the question…are we reaching saturation of midlevel providers?
My prediction is that I think we are going to be approaching saturation soon for large cities, if we are not there already. The rural areas will most likely always struggle to fill positions unless reimbursement changes to make it more attractive to practice there.
As independent practice of NP’s expand to even more states, we will see increased competition to push costs lower. Even though independent practice is not allowed in my state, there are 8 NP only practices within a 10 mile radius. They range from dermatology, to primary care, HIV care, to psych practices. Some tele-medicine companies are now 100% run by midlevels only.
The Future Of Avoiding Super-Specialization
As midlevel providers continue to rise, I think that we will see some fellowships die out. Maybe not completely, but some fellowships will be severely hurt in their ability to attract physicians.
For example, why go to medical school plus 3 years of family practice and then a year long hospitalist fellowship when a NP can replace that physician without all the training?
The desire to go to one of these fellowship programs is going to drop severely. I would bet that obesity medicine (weight loss clinics run by midlevels), HIV clinics (there are already 2 HIV + NP only clinics in my city), community medicine, geriatric medicine, hospice etc… will all be severely affected. Nurse practitioners can easily slide into these types of roles without extra training. The financial loss of missed income for 1 year of one of these fellowships will make them much less attractive to physicians in the future.
Anything procedure related will have much more of a moat that will protect them from encroachment.
What The Future May Look Like For Employed Physicians
The rise of the midlevels is here. The previous hospital I worked for had a hospitalist group that fired all the under preforming doctors and replaced them with midlevels at a lower cost.
I suspect there will be more pressure on doctors to bring in revenue to support their physician salary. There could be a risk of replacement with a midlevel if a doctor is under preforming. Don’t think this will happen? There are examples of this already happening all over the county.
My suspicion is that nurse practitioners will continue to encroach on outpatient non surgical based practices in the coming years. I suspect that this will lead to increased competition, driving down the price of delivery of healthcare to patients in the outpatient setting.
With increased competition, expect to see more specialized non specialist. For example, non-dermatologist/ plastic surgeons opening up med spas. I would also expect a modest drop in salary for employed non procedure based physicians over the next 10 years.
What are your thoughts?
Remember that these are my best guesses based on where I see the market going in the future.
Such a great article. Advanced Practice Clinicians (APC’s, aka midlevels) are gaining a stronger foothold because medicine is becoming more and more workflow or algorithm based. That’s why a lot of AI is focusing on the healthcare space. The reason the VC’s are putting up cash for AI in healthcare is because there is very little thinking in patient management – it’s mostly workflows which can be programmed into a machine learning algorithm.
The specialty space has also become so expensive that it was ripe for takeover by APC’s. Much like healthcare was ripe for takeover by HMO’s in the 70’s/80’s.
At the same time, there are physicians who are exiting this space and catering to the biohackers and those who can tell the difference between intelligent care and cookie cutter care.
So long as a patient just wants a medication or an order for a lab test, they will always choose the cheapest option, such as APC’s. Once that saturation point hits, as you mentioned, the marketplace will become a lot more divided.
Data transparency might be helpful; it’ll either highlight the outlier clinicians to be mostly physicians or it’ll show that a computer can do as good of a job as any APC or MD/DO – in which case the lower-cost option should suffice.
Unfortunately medicine is starting to become a bottom line business. Administration would rather have more mid levels who are less expensive being supervised by just a handful of physicians.
There is potential for the need for physicians to drop as more and more of their clinical duties are being handled by mid levels at lower costs.
Are there any specialties that you recommend medical students avoid in concerns of job prospects with so many nps?
As a “older” NP of 20 years I can see the concerns that medical students face. I personally do not endorse all-online education of midlevel providers as this takes away from quality of the new graduate APP. The in-person program I completed was a detailed curriculum and the washout was significant. (Out of 36 that began the program, 6 of us finished) I am also very distressed at the DNP programs that offer nothing towards advancing the clinical role of the APP. I have specialized in ENT services and I have been very fortunate to have an excellent professional relationship with the physician I collaborate with. I also will collaborate with many other professionals on a regular basis to be able to take care of my patients appropriately. I would like to say that we are not “encroaching” upon territory, but adjunct to patient care. APP’s are now also starting to realize that corporations are taking advantage of them and many NP’s can make more money as a floor nurse than in an outpatient setting. We are already at saturation for my area I live in- competition for a position is fierce and the new APP’s are being passed over for seasoned mid levels. f We are striving to make appropriate changes among ourselves as APPs that reflect knowledge and competence. Good article.
I stopped reading at this article’s title. Stop referring to advanced practice, licensed independent practitioners as “midlevel providers” and “midlevels.” It’s an old, demeaning reference and quite frankly, inaccurate and meaningless.
In relation to a physician, is an NP considered an advanced practice provider? I do not think so. What services does an NP provide that a physician cannot? An NP provides a mid-level range of services in relation to what used to be the only provider category — the physician. Thus, historically and forevermore, an NP will always be a mid-level provider.
That nurse practitioners, PAs etc are midlevels is complete common sense. No idea why anyone could not understand this when seeing the facts
How do you like “physician extender?”
If you are a doctor you should consider joining the AMA. it is the only organization out there representing all physicians and medicine as a whole.