
Since January 2021, billing rules have changed for CMS (Medicare) and most insurance companies. Billing is now primarily based on time or medical decision making for outpatient clinic visits. Historically there have been 5 levels of care, with level 5 being the most complex visit. Up until 2021, almost all of the codes used for outpatient medicine were level 3 through level 5. Level 3 visits are often quick, easy, and straightforward visits. Think a sore throat that is caused by a virus and a doctor telling the patient to take over the counter meds only.
While level 3-5 visits are still most of the visits, you will see why level 3 visits are starting to become more and more rare (at least in our clinic). At the end of the year, I went over all of our billing metrics. I could not help but wonder where all the level 3 visits have gone in our billing reports. Seems like after a bit of digging and though, I figured it out.
Changes To Billing Codes
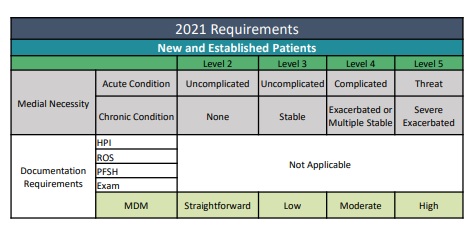

First change: Level 1 codes were discontinued January 1st, 2021.
Another very positive change with the 2021 update is that the day of the visit, all time spend on that visit is counted. The time that was spent looking in the chart notes, talking to a consultant, or filling out paperwork adds to the time. Previously, it was time only spend on direct patient contact.
The physical exam and review of systems no longer significantly affects the level of care. I think we can all agree that trying to do 12-point review systems for someone who comes into your clinic who might be having a heart attack might not be totally relevant. Yes, I hear you about the crushing chest pain but how have your allergies been lately?
Why Level 3 Visits Have Evaporated
There are three reasons why we are billing for far less level 3 visits now compared to in the past.
- The rise in competing telemedicine services, sometimes very low cost or free to the patient with 24/7 availability.
- Patients are much more complex, often times with concurrent mental health problems (anxiety and depression) that takes up a large portion of the visits.
- Due to patient portal, some of these visits that used to be very quick visits are now answered via portal.
These are the three biggest reasons why we have noticed that our visits for level 3 visits have almost completely gone away. I remember when I was younger my PCP used to make me come into the office when I was a kid to follow up on my blood work. I would hear everything is normal, go over the labs, and be out of the office in about 5 minutes.
Now that happens virtually via a message through the portal. Even mild abnormalities are noted via the portal via a template response. Hi patient. You are prediabetic, here is some info about what this means and what you can do about it, schedule follow up if you have more questions and I would like to see you again soon to see how this improves.
Telemedicine
Don’t get me wrong. The rise of telemedicine has been a wonderful addition to the clinic. Telemedicine has helped many small offices survive the pandemic. Heck, it helped my clinic survive the pandemic.
However, this rise has also led to a lot of competition in medicine. This ranges from other brick and mortar practices offering telemedicine to online only options. We have noticed that many of our competitors are now taking those easy level 3 visits virtually that we used to see in office.
Pre pandemic about 20% of our visits would be a level 3 visit, also knows as a low complexity visit. Post introduction of COVID-19 to the world, about 2% of our visits are now Level 3 visits.
The easier, quick visits seem to have evaporated from our practice.
Patients often tell us that they did a quick $20 online visit to talk to a different doctor for their UTI and didn’t even bother calling us since they could do the visit at their convenience anytime of the day or night.
Why Don’t We Offer 24/7 Telemedicine
This is something that we’ve contemplated with for a long time now. Instead of our patients getting telemedicine services elsewhere, why don’t we simply offer these services 24/7 to our patients?
The answer is purely financial. Paying a nurse practitioner or physician assistant over $100,000 a year to take after hour calls for Level 3 visits does not really financially make sense.
Average reimbursement for a level three visit can be as low as $50 for small practices. Assuming $50 per visit, that nurse practitioner or physician assistant would have to do about 2100 encounters just to pay their salary. Overhead is going to also be expensive with malpractice insurance, EMR costs, etc. The PA would have to do about 15 visits a day just to pay overhead and their salary before any possibility of profit could occur.
We are not in a position right now where we can take this kind of possible financial loss as a premium service for our patients.
Length Of Visits Has Expanded
It is really tough to have short visits under 20 minutes face to face now. Many times, we struggle to even hit a 30-minute cutoff for some patients.
It seems now more than ever, many of our patients are coming in quite ill. Or our patients are coming in with many issues they need discussed. Most of the time there is concurrent depression or anxiety that in now confounding their health ailments. This all takes a lot of time to go through. Much more time than before.
Outpatient medicine was already hard, and now having a day full of longer tough visits is a bit taxing on our doctors. We do fit in telemedicine quick visits during the day, but again, if a patient doesn’t like our timeline, we notice that they simply go elsewhere to get their quick medication online.
Virtual Is The Future
The cat is out of the bag on virtual medicine and there is no going back.
Our patients can now book dietitians online, they can do therapy online, and they can even get same day delivery to their house of their prescriptions including controlled substances. We have moved to a concierge level of service with telemedicine to every patient. Patients often times do not even have to leave the house anymore to seek medical care. Now, how good quality this care is, that is a whole different topic.
We all have to adapt to this new normal.
Limitations With Virtual
Virtual visits often times feel “good enough.”
There is so much that is done in the office that gets skipped with virtual visits. We are finding those issues that get “missed” being addressed way too late.
For example, one patient has not physically been back into my office in 2 years. When he came back into the office, we found out that he gained 85 pounds. He also noted normal blood pressure at home during our virtual visits. Our office our readings were in the 190s for his systolic value on multiple repeats.
Now, this does not happen to every patient, but it is a big limitation of virtual visit only.
We have found that some things worked well for virtual visits. Mental health visits for example. These visits work often wonderfully virtually. Acute sick visits, these are just very tough virtually. I can’t take vitals or examine the area of concern. It is very much a “good enough” kind of visit. That is why we have put limitations on what visits can and can not be done virtually.
Future Of Medicine
It pains me to type this, but I do think that the future of medicine is most likely going to be a subscription service on top of your insurance.
It pains me because I already pay, in my opinion, insanely high premiums for health care. The idea of paying yet even more for a yearly subscription is a hard pill to swallow.
The benefits of having insurance seem to be eroding more and more every year. My premiums keep going up, and my coverage seems to keep going down.
The group that offers the most “amazon like” service will most likely win first. Patients want visits now, they want meds shipped right to their door same day, and they want access 24/7. The race to low cost online care is well on its way.
YouTube
My second video while trying to mirror one of my posts. Learning a bit more about adding music, transitions.
Thanks for following along!
Any considerations to slowly transitioning to exclusively being subscription based and getting rid of all insurance?
It is something that we considered but right now, no, we plan on continuing to take insurance. The growth is just so much faster compared to if we do not take insurance. Our plan is to grow as fast as we can without taking any external money and to see how big we can make the group. We are going to add on a premium level subscription in the near future. Still working with my lawyer on the details about that. Stay tuned!
Thank you for this post, I was thinking about it all day, as I saw one complicated patient after another, with maybe one true level 3 for the whole day.
The struggle is real. I miss the quick visits for a big of a break between the complicated visits during the day.
CMS offers remote patient monitoring (RPM) for chronic conditions (CPT 99453, 99454, 99457, 99458). This is the telehealth version of “Easy Level 3 Visits”. For example, you order patients with hypertension to be monitored through RPM until they meet their treatment plan objective, which can be months.
Next, outsource the daily operation (RNs, MAs for billing, patient education, engagement, etc.) to a 3rd party managed services company like https://www.willowhealthrpm.com. They charge per patient per month, with no minimum. That way you can offer this service to your panel without incurring additional labor cost. Let me know if you want to know more details.